Resident Case report
Case Report – When R Meets T
OHSU Resident – Ethan Kimball, DO, MS, PGY-2
Case:
An 18-year-old male is brought to the emergency department via ambulance after
being found unresponsive with agonal respirations at home. Per EMS report, the
patient was pulseless on arrival and CPR was initiated. During the initial
resuscitation, he received naloxone, and was defibrillated once for pulseless
ventricular tachycardia with subsequent return of spontaneous circulation. In the
emergency department, he was thrashing, screaming, and unable to follow
commands. Given his significant agitation, restraints were placed and 10mg of
intramuscular Olanzapine was administered. IV access was then established and he
required an additional 4mg of intravenous lorazepam in order to achieve adequate
sedation.
The patients’ mother stated that prior to this event, he was in his normal state of health and had never had an episode like this before. She denied any known ingestions or drug use other than marijuana. However, he had lost 50lbs over the past month in the setting of decreased appetite, abdominal pain, and nausea. On further review of his chart, he presented to the ED multiple times over the past month for the above complaints. His prior work-ups were significant for a normal scrotal ultrasound and abdominal/ pelvic CT, as well as one episode of hypokalemia requiring replacement.
Vital Signs:
Temp: 97F, BP: 111/53, HR: 93, RR: 20, O2 sat: 98% on room air
Exam:
Gen: Agitated, intermittently consolable, mumbling incomprehensible words
HEENT: Atraumatic, Pupils 5mm bilaterally, PERRLA, EOMI, and no nuchal rigidity
Resp: Clear to auscultation bilaterally, no wheezes, rhonchi, or rales
CV: Rapid rate, regular rhythm
Abd: Soft, non-distended, non-tender
Neuro: CN II-XII intact, able to move upper and lower extremities, exam limited by patient’s inability to cooperate
Initial work up included:
CBC, CMP, UDS, urinalysis, lactate, APAP, Salicylate, EtOH, and ASA levels. Additionally, blood cultures, an EKG, CT brain without contrast, and lumbar puncture were obtained. He was started on acyclovir, vancomycin, and ceftriaxone to cover empirically for meningitis/encephalitis.
EKG:
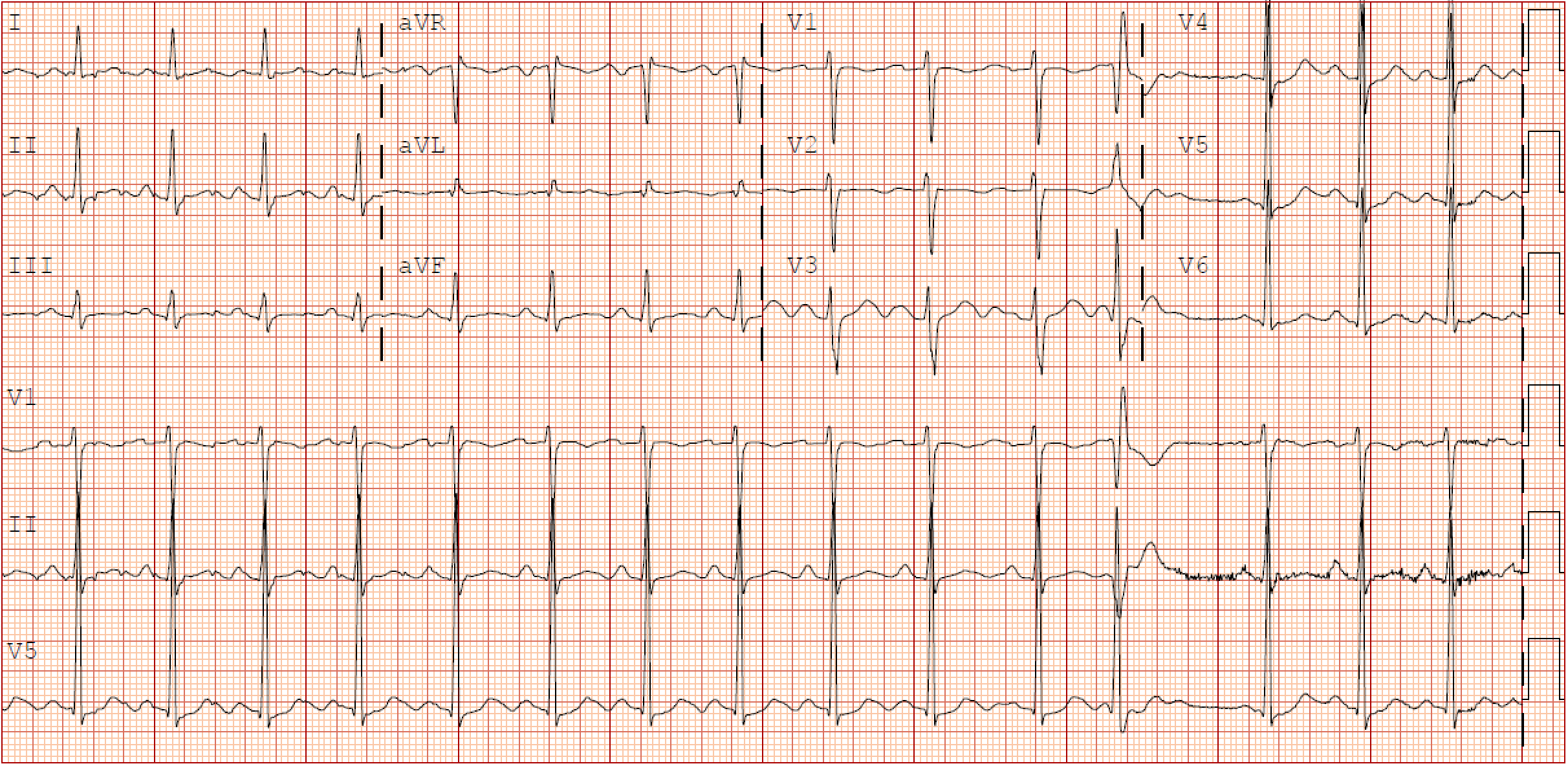
Interpretation:
Sinus rhythm, HR 93, PR 104, QTcB 515, QTcF 472
Diagnostic results:
Laboratory work-up was notable for a leukocytosis of 15.8 x109/L, lactate of 7 mmol/L, glucose of 214 mg/dL, trace ketones in the urine, and positive UDS for Cannabinoids/THC and opioids.
All other labs were within normal limits and imaging was unremarkable.
Follow up:
The patient was admitted to the PICU for close monitoring and further work up for altered mental status of unclear etiology. An EEG was obtained and there was no evidence of seizure activity. On further questioning, the patients’ mother admitted to giving him a Norco for abdominal pain at home, which could explain the positive opioid UDS. Repeat EKGs continued to show prolonged QT intervals ranging from 509ms to 619ms. He remained intermittently agitated, however he was consolable and his mentation returned to his normal baseline. Due to low concern for infectious etiology antibiotics and antivirals were discontinued. He was maintained on telemetry, where he was noted to have frequent pre-ventricular contractions.
On hospital day two, the patient spontaneously went into a polymorphic ventricular tachycardia that was recorded on telemetry (figure 1). During this episode the patient had agonal respirations, absent pulses, and a code blue was called. Defibrillation pads were placed, and CPR was initiated for a brief period. Just prior to defibrillation, he converted back to a normal sinus rhythm. His mother was at his bedside during this event and informed the medical team that his presentation was similar to that of when he was found unresponsive at home. He was started on an intravenous lidocaine infusion and oral nadolol to promote cardiac membrane stability. Strict electrolyte parameters were also established to maintain ionized calcium above 1.2, potassium greater than 4, and magnesium of 2. All QT prolonging medications were withheld. The patient had resolution of his PVCs and there was no recurrence of ventricular tachycardia therefore lidocaine was weaned off after 48 hours. His QT duration on subsequent EKGs remained prolonged and the patient was ultimately discharged with a wearable external defibrillator “LifeVest” and a plan to follow up with cardiology for placement of an internal cardiac defibrillator (ICD).

Figure 1.
Telemetry monitor showing an initial narrow complex QRS with pre ventricular contractions that abruptly converts into a polymorphic ventricular tachycardia with oscillatory changes in amplitude around an isoelectric line consistent with torsade de pointes.
Discussion:
Long QT syndrome is an uncommon but life-threatening condition that must be considered in young patients presenting with a dysrhythmia, especially ventricular tachycardia. It has been estimated to cause up to 4,000 cases of sudden cardiac death per year in children and young adults1. Given the nonspecific presentation, long QT syndrome often goes undiagnosed until a patient presents with sudden cardiac arrest. Half of all people who have this syndrome will experience their first abnormal cardiac rhythm by the age of 12, and 90% by the age of 401.
A normal QT duration is generally accepted as less than 440ms; however, some sources argue that women naturally have a longer QT duration and up to 460ms is acceptable. If the QT duration is greater than 500ms there is an increased risk of torsade’s de pointes. Between 440ms and 500ms is a grey area where most providers only consider a patient at risk if they are symptomatic or have concomitant cardiac arrhythmias2.
The QT duration is defined by the time from the start of the Q wave to the end of the T wave when the heart rate is 60 bpm. There are many ways to calculate a corrected QT duration (QTc) for a heart rate that is not 60 bpm; two common calculations used are the Bazett and Fridericia formulas. The Bazett formula is QTc=QT/√RR, which is the most commonly used, however will over-correct at heart rates over 100 bpm, and under-correct at heart rates less than 60 bpm. The Fridericia formula is QTc=QT/RR1/3 and is considered to be more accurate when the heart rate is less than 60 bpm or greater than 100 bpm3. It is important to use the most appropriate formula to correct for the QT duration to ensure diagnostic accuracy.
QT prolongation has a large differential and requires a thorough workup before diagnosing a congenital or idiopathic cause. More than fifty medications have been identified as a potential cause of QT prolongation, making a complete medication list important1. Additionally, electrolyte abnormalities specifically hypokalemia, hypomagnesemia, and hypocalcemia can prolong the QT duration; these may be caused by starvation states, anorexia, restrictive diets, as well as medications such as diuretics4. Medical causes such as hypothyroidism, myocardial infarction, severe bradycardia/ AV block, and hypothermia can also lead to a prolonged QT duration5. In the emergency department it is important to identify patients with a prolonged QT, consider their level of risk for dysrhythmia, and establish an appropriate disposition for further work-up.
In our specific case the patient was severely altered in his post-resuscitative period. He was determined high risk and required ICU level care for close observation and further work-up. The patient had multiple exacerbating factors as well as an underlying pathology that led to his dysrhythmia. He had recently been taking Zofran and was administered Olanzapine, both of which are known to cause QT prolongation. The patient had poor dietary nutrition for over a month leading to electrolyte derangements that required multiple replacements of calcium, magnesium, and potassium during his PICU stay. These factors in addition to his baseline long QT duration put him at an increased risk for R on T phenomena leading to his episodes of torsade de pointes. Due to the immediate actions taken by EMS, appropriate disposition in the emergency department, and thorough work-up in the PICU, the patient was safely discharged with appropriate follow up for ICD placement.
References:
- National Health Institute: Long QT Syndrome. https://www.nhlbi.nih.gov/health-topics/long-qt-syndrome. 2021
- C. Clark, MD. The Pediatric EKG and Long QT Syndrome. EMRA. https://www.emra.org/emresident/article/pediatric-ecg. 2018
- E. Burns, R. Buttner. QT interval. Life in the Fast Lane. https://litfl.com/qt-interval-ecg-library. 2021
- C. Berul, MD. Uptodate.com: Acquired long QT syndrome. https://www.uptodate.com/contents/acquired-long-qt-syndrome-definitions-causes-and-pathophysiology. 2021
- M. Ackerman, MD, PhD. Consultation with the specialist: Long QT syndrome. Pediatrics in review Vol 19 No. 7. 1998
ACEP updates
1. ACEP released a statement on the new interim final rule (IFR) to implement surprise billing legislation. “Emergency physicians are profoundly disappointed that the Administration’s IFR is almost entirely inconsistent with Congressional intent to create a fair and unbiased process to resolve billing disputes.” Read the full statement.
2. ACEP was recognized with a 2021 Summit Award by the American Society of Association Executives (ASAE) for the ACEP COVID-19 Field Guide: A Valuable Tool for Frontline Clinicians. Check out the video.
3. The countdown is on until ACEP21 in Boston. If you can’t be there in person, the at-home package lets you still be part of the action from wherever you are. Your meeting, your way.
4. Asynchronous testimony on all resolutions assigned to a Reference Committee (Resolutions 10-77) is now open to all ACEP members until Oct. 14.
5. New Podcast: Lineus Medical is simplifying and preventing the dislodgement of peripheral IVs. The podcast explains how this simple device can save time, reduce complications and improve workflow issues associated with peripheral IV dislodgement.
6. New EMF grant opportunity! EMF and the National Institute on Drug Abuse announce the EMF/ NIDA Mentor-Facilitated Training (MFT) Award in Substance Use Disorders Science Dissemination. The award funds up to $10k for the trainee stipend and up to a $2k stipend for the mentor. Proposals due Nov. 12.
7. HeART of EM: We are celebrating our members’ talents at ACEP21 through a virtual art gallery showcasing your art, music, video, storytelling, spoken word, comedy and everything in between. Upload your submission by Oct. 15.